




Treatment Journey
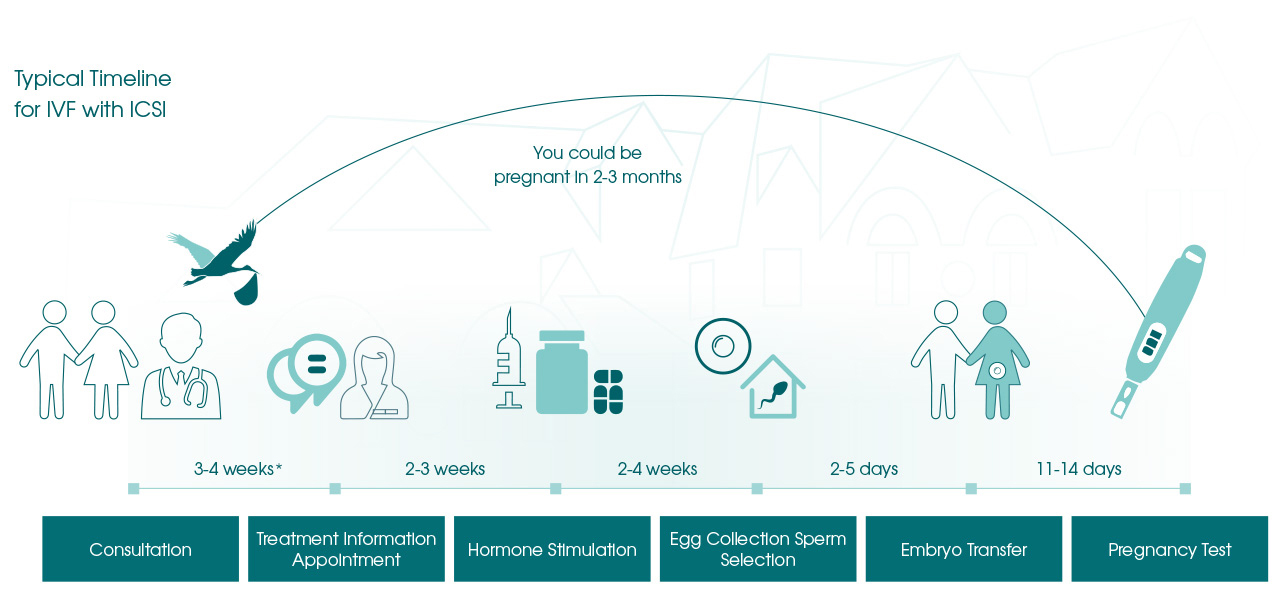
Most assisted pregnancies follow a carefully structured fertility treatment journey, as shown in the steps below.
Consultation
Every treatment journey begins with an initial consultation with one of our medical Consultants
At the initial consultation, we would like to meet you and your partner (unless you are considering becoming a Single Parent) to help us obtain a full medical history. As an independent clinic, it is a requirement that your Body Mass Index (BMI) must be under 34 at the start of treatment to ensure your safety during sedation.
This will include details of any previous fertility investigations or pregnancy history. We need to know if either partner already has children. Please be reassured that we will provide the same help and support with your second or third child as we will with your first.
Your initial consultation at the Herts & Essex Fertility Centre marks the start of your treatment journey with us. It is an opportunity for a thorough discussion of your situation with one of our Fertility Consultants.
The appointment with the Consultant lasts for about an hour, which allows plenty of time to discuss in detail both your medical histories and the implications of assisted reproduction for each of you. Prior to your meeting with the Consultant, a nurse will undertake some baseline observations.
Dr Lucy Richardson talks about the key points in a typical fertility journey through the laboratory and the science behind fertility treatment in this video.
We will identify and discuss in great detail the fertility treatment options most suitable for you, with your particular circumstances in mind. We will offer you our expert opinion and point out everything you need to consider when you are making your decision, including the risks involved and the chances of success under your circumstances.
You could get a referral from your GP, but it is not essential. However, if you wish us to correspond with your GP or Consultant it is a Human Fertilisation and Embryo Authority (HFEA) requirement that you sign a consent form to that effect. It is likely that your GP/Consultant has already performed preliminary investigations and it is important for us to see the results, even if we may repeat some of them. We will discuss the implications of these results with you at this appointment.
We will assess your lifestyle. This will include your diet and weight, whether you do enough exercise and if you smoke.
At this stage, we will discuss the treatment options that are likely to be most successful for you. We will give you our candid opinion of the risks involved and your chances of success.
Do ask as many questions as you wish, and remember we are here to help you make the right choice.
If you would like to go ahead, we may be able to begin your treatment as early as your next menstrual cycle, provided that your fertility assessment (AMH tests and semen analysis) and screening tests (HIV, Hepatitis B and C, etc) are completed and the results available for consideration.
Fertility and your weight
Your Body Mass Index or BMI calculator is a measure of health, based on an individual’s weight and height.
For women, being underweight, overweight or obese can have a profound effect on ovulation and therefore your ability to conceive. Some women may suffer from hormonal disorders which cause them to ovulate infrequently or not at all. This not only reduces the chances of conceiving naturally but also means fertility treatment, such as IVF, is less likely to be successful.
Infertility is also more prevalent among men with higher BMI values. Male body fat is closely associated with the production of male reproductive hormones. Too much or too little body fat disrupts hormones and can affect testosterone and oestrogen levels. Any changes in hormones can affect sperm and its production. Being overweight or obese can reduce a man’s sperm count, and sperm motility and quality.
As a general rule, we don’t allow starting IVF treatment until you have a BMI of between 20 and 34.
Click here to find out more about Why does BMI matter?
Your initial consultation at the Herts & Essex Fertility Centre marks the start of your treatment journey with us. It is an opportunity for a thorough discussion of your situation with one of our Fertility Consultants.
This usually lasts about an hour, which allows plenty of time to discuss in detail both your medical histories and the implications of assisted reproduction for each of you.
We will identify and discuss in great detail the fertility treatment options most suitable for you, with your particular circumstances in mind. We will offer you our expert opinion and point out everything you need to consider when you are making your decision, including the risks involved and the chances of success under your circumstances.
Saline Infusion Sonography (SIS)
What is SIS?
SIS is a quick procedure used to detect any abnormality inside the uterine cavity such as polyps (small growths of endometrium), fibroids or adhesions (scar tissue).
Show more
During a transvaginal ultrasound scan a small amount of sterile saline solution is injected into the uterus via a small catheter. SIS is advisable for the female partner before any fertility treatment to confirm that the uterus is in a good condition for embryo implantation.
SIS is normally done at the same time as the Pipelle procedure, usually within a week before the start of your treatment. It is important that you are not pregnant at the time, so you must abstain from intercourse or use effective contraception during that cycle.
Please note that SIS cannot be performed if you have Pelvic Inflammatory Disease (PID).
Show less
Screening
Screening
Your health, and the health of your future child, will always be of paramount importance to us. Certain conditions can have serious consequences for mother and baby, so every patient – male and female – who chooses to have fertility treatment with us will be required to undergo specific screening investigations as laid down by the Human Fertilisation & Embryology Authority (HFEA) Code of Practice.
Those screening tests are as follows: HIV, Hepatitis B, Hepatitis C, Chlamydia and Gonorrhoea. We will need the full results back from the screening before we can start your treatment.
It is worth remembering that a positive result for one or more of these diseases does not necessarily mean that you cannot have fertility treatment – and cannot start your family – but it might mean that we have to approach the treatment with various safeguards in place.
We will talk you through all the implications of having these tests at the initial consultation, but if you have any queries or concerns at any stage you can always speak to a member of our nursing staff. They are friendly, approachable, non-judgemental and, above all, extremely experienced and knowledgeable.
When and where will screening take place?
After your initial consultation, you will need to make an appointment with a nurse coordinator to have both partners’ blood tests done here at the Herts & Essex Fertility Centre. This can be done at your Treatment Information Appointment (TIA) when you are ready to start treatment. Screening needs to be dated within 3 months of starting treatment.
You may have your screening carried out elsewhere but this must be through a UKAS accredited laboratory and you have the responsibility to ensure we have the results from the laboratory prior to starting your treatment. Once you have had an egg collection, these screening results become valid for two years.
Treatment Information Appointment (TIA)
When you are ready to begin your treatment, we will arrange a Treatment Information Appointment (TIA) for you to see one of our Nurse Coordinators
Unlike other clinics, at Herts & Essex Fertility Centre each patient is treated as a unique individual and for this, we offer an appointment about an hour long with a Fertility Nurse on a one-to-one basis, prior to starting treatment.
This appointment gives you the opportunity to raise any concerns in complete confidence. The nurse will talk you through the treatment procedure recommended by the doctor step-by-step, and demonstrate how to self-inject any drugs, if necessary. Most of the fertility drugs we prescribe are given by subcutaneous injection – often abbreviated as “subcut” – which is an injection beneath the skin, usually administered into lower abdomen or upper thigh similar to the diabetic insulin injection.
Show more
This gives you the opportunity to study all the treatment consent forms with a fertility expert, and to ask as many questions as you want in complete privacy before you sign the forms.
Your fertility treatment cannot begin until relevant consent forms are completed and signed, as this is a legal requirement of the Human Fertilisation and Embryo Authority (HFEA) which regulates all IVF clinics in the UK.
It is at this appointment that we will give you a provisional programme of dates for your treatment appointments so that you can arrange any time off work, should you find it necessary.
This appointment is your chance to ask as many questions as you want – we want you to be fully informed so that you feel confident, comfortable with your decision and the course of fertility treatment you are about to undertake.
We ask that both you and your partner visit the online consent platform and take your time to read through and complete the HFEA Consent Forms. We shall explain these forms in full again at the appointment and then ask you to sign them. Your fertility treatment cannot proceed any further until these forms are completed and signed. This step is a legal requirement of the Human Fertilisation & Embryology Authority (HFEA) which regulates all IVF clinics in the UK.
Show less
Ultrasound Monitoring
Ultrasound scan
By now, you will have received details of all the necessary medications you need and been allocated to one of two different drug protocols, the Long GnRH Agonist Protocol or the Short Antagonist Protocol.
The Long Protocol otherwise known as “down regulation” makes your ovaries temporarily inactive which promotes easier management of your treatment cycle during stimulation by daily hormone injections. This protocol is used in women who have normal ovarian reserve. You will need an ultrasound scan to confirm that the down regulation has been successful.

Show more
In the Short Protocol, there is no down regulation, and it is reserved mainly for women who have poor ovarian reserve. It is also used sometimes in women who have a high ovarian reserve as a means of reducing the risks of ovarian hyperstimulation.
In both protocols, you will need daily Follicle Stimulating Hormone (FSH) injections to promote the development of multiple follicles in the ovaries.
Regular ultrasound scans will help us see just how well your ovaries are responding to the injections, by counting and measuring the size of the developing follicles and the thickness of the endometrium (the inner lining of the womb).
Human chorionic gonadotropin (hCG): the late-night injection
Once your follicles and endometrium are at the optimum stage of development, you will be given an injection of Human Chorionic Gonadotropin. hCG is a hormone that will induce the ripening of your eggs so that we can collect them about 36 hours later, just a few hours before they are naturally released by your ovaries.
Why do we call it the late-night injection?
This is because the injection is usually given between 9pm and 1am; a time chosen to correlate directly to the exact time of your egg collection some 36 hours later.
Show less
Egg Collection
On the day of egg collection both partners will need to attend the unit. Today we will harvest your eggs and prepare the semen sample for insemination, which will take place later in the afternoon.
The egg collection procedure will take approximately thirty minutes, after which you will be cared for by our specialist nursing team.
Shortly after returning to recovery your partner or family member/friend will be able to join you. Expect to be at the clinic for 2-3 hours on Egg Collection Day.
Before you return home you will be seen by your consultant and provided a laboratory guide that details what will happen over the forthcoming days as your embryos develop. An embryologist will then call you later in the day following the insemination of your eggs. During this call, they will confirm with you the number of eggs collected, the quality of the semen prepared, and the chosen method of insemination.
IVF or ICSI?
During your initial consultation, we would have discussed the results of the semen analysis and both partners’ reproductive history. Those factors will help us choose one of the following fertility treatment options – IVF or ICSI – for fertilisation of your eggs.
- In-Vitro Fertilisation – IVF
- Intra-Cytoplasmic Sperm Injection – ICSI
IVF and ICSI are laboratory techniques by which a single sperm fertilises a single mature egg. The decision as to which treatment is the most suitable for you will depend on the quality of the sperm sample you provide on the day of the egg collection. Sperm quality can fluctuate on a regular basis.
Click here to find out more about In-Vitro Fertilisation – IVF
Click here to find out more about Intra-Cytoplasmic Sperm Injection – ICSI
Click here to find out more about Surgical sperm retrieval – PESA and TESE
Embryo Development
The laboratory will contact you daily with updates regarding your embryo development, right from the morning after your egg collection.
In order to optimise the development of your embryos, your fertilised eggs are left to develop in the controlled environment of the incubator following a process known as undisturbed culture.
An embryologist will call you on Day 1 to inform you how many of your eggs have fertilised normally. Depending on the number of eggs that have been fertilised, your transfer will be scheduled for either Day 3 or Day 5 of culture. The embryologist will confirm the plan for your embryo transfer during your Day 1 phone call.
Show more
If you are having a day 2 or 3 transfer, with your permission, all excess embryos will be cultured on to day 5 or 6, to see if they are able to progress to the blastocyst stage at which time they may be frozen if they are of good quality and contain the visible and necessary structures known to give rise to a pregnancy.
The embryologists will call you daily (with the exception of day 4 when no embryos are assessed) by 10am each morning. The Laboratory Guide given to you on the day of egg collection will provide a good insight into the journey your embryos will make in our laboratory, providing information and pictures to help you understand how we make our decisions regarding both the number of embryos to transfer and the stage when the transfer is made to maximise your chances of success.
We strongly believe that embryo/s should be replaced at the optimum stage of development when they have proven themselves through a process of self-selection. It is for this reason that we perform embryo transfers 7 days a week, on days 2, 3 and 5.
Show less
Embryo Transfer
Embryo transfer is the process by which your developing embryo/s is transferred into the uterus.
This occurs 2-5 days after egg collection and will be determined by the number, development, and quality of your growing embryos. The embryologist will guide you when you need to attend the clinic for embryo transfer.
The procedure itself is usually simple and straightforward without the need for anaesthetic, very similar to a female cervical smear test. During the procedure, we insert a soft catheter into your vagina, passing through the cervix into the uterus. Once the catheter is in place, we expel the embryo/s into the uterus.
Show more
Prior to the embryo transfer taking place, you will have the opportunity to speak both with the clinician and an embryologist, who will discuss your embryo development and the number of embryos for replacement and subsequent culture/freezing. The decision regarding the number of embryos able to be replaced is governed by our regulatory body, the Human Fertilisation and Embryology Authority (HFEA), with a maximum of two embryos permitted for female patients under 40 years of age, and a maximum of three for those over forty. Patients undergoing a cycle of egg donation are permitted to have a maximum of two embryos replaced irrespective of their age. For those patients, at the highest risk of a multiple pregnancy, the recommendation is to have a single embryo transfer (SET) if their embryos reach the blastocyst stage. For this select group, the replacement of one blastocyst will not have any significant impact on the excellent chance of success but will instead safeguard both mother and baby from the risks of a multiple pregnancy and optimise the chances of you delivering a healthy baby. Remember though, having been fully informed, the ultimate decision on the number of embryos to be replaced rests with you the patient.
At the time of embryo transfer, you will have the opportunity to observe your embryo/s on the theatre monitor. We are also able to take photographs which you are able to take home should you wish. The embryologist will give you an information sheet summarizing your treatment and detailing when your pregnancy test is due. You can also refer to your laboratory guide for advice and information during this time as you lead up to your pregnancy test.
Embryo freezing
Stimulation of ovaries to promote egg production during fertility treatments often result in more embryos being created than what can be transferred into your uterus in the same treatment cycle.
Embryo freezing (Cryopreservation) is available to patients who have excess good quality embryos which have reached the blastocyst stage either on day 5 or 6 after egg collection. With few exceptions, we only freeze embryos that have reached the blastocyst stage, in order to maximise your chances of success in a later Frozen Embryo Replacement cycle (FER). It is only at the blastocyst stage that we are able to determine the presence of and assess, the structures necessary to give rise to pregnancy: a group of cells that will give rise to the fetus, the Inner Cell Mass (ICM) and cells which will form the placental cells, the Trophectoderm.
Both partners will need to give permission if they wish to consider freezing suitable and surplus embryos. The Nurse Coordinator will help you complete the necessary consent forms at your Treatment Information Appointment (TIA) at the commencement of your treatment cycle. Freezing your excess good-quality embryos will give you the opportunity to return for a Frozen Embryo Replacement (FER) cycle at a later date, hopefully when trying for more children, or alternatively if your fresh treatment cycle has failed. The Frozen Embryo Replacement cycle has the benefit that the embryos are thawed and replaced into the uterus at the same corresponding stage in the cycle as when they were frozen, this time without the need for ovarian stimulation or egg collection.
At the Herts & Essex Fertility Centre we use the method of vitrification to cryopreserve or freeze suitable blastocysts. This latest technique serves to rapidly cool the embryos, leaving them free from ice crystals that can otherwise damage their structure. This method of freezing enables 80% of patients to progress to embryo transfer in a Frozen Embryo Replacement cycle.
Show less
Treatment Outcome
Your pregnancy test will be in approximately two weeks from the date of egg collection. We will advise you at embryo transfer of the date for your test, and for this test, the first morning urine sample must be used to ensure an accurate result is given.
You can purchase a pregnancy test kit from a local pharmacist; we recommend a non-digital test kit be used. There may be circumstances where a blood test is necessary or indicated, and we will advise you accordingly at embryo transfer should you need to attend the clinic for a blood test.
If your pregnancy test is positive you will need to continue with your prescribed medication, and we will make you an appointment for an early ultrasound pregnancy scan at the clinic in a further 3-4 weeks. If, however, the test is negative, as soon as you are ready, we will book you a follow-up appointment with one of the clinicians to discuss your cycle, answer any questions you may have and suggest future plans.
Show more
The time between the embryo transfer and the pregnancy test can be the most difficult, as you wait to find out the outcome of your fertility treatment. Some patients describe a feeling of being in limbo and many find that the days seem to pass by slowly. While there is no formal contact with the clinic staff at this time, we understand how difficult this wait can be. In addition, the odd twinge and those little aches and pains that can be worrying even during a routine pregnancy take on an even greater significance during assisted pregnancies. So, if you have any questions, or if you just need some reassurance that all is well, you’re more than welcome to phone in and speak with one of our nurse coordinators. A calming, friendly voice from someone with years of fertility experience at the other end of the telephone can be comforting.
Please remember, we are more than happy to be a comforting voice, so you can call us at any time: 01992 78 50 60.
Show less