




13th March 2023
Endometriosis and infertility
David Ogutu MRCOG
Medical Director and Consultant Gynaecologist
![]()
Follow the latest news and developments in the world of fertility.
< View all our fertility news and posts
13th March 2023
David Ogutu MRCOG
Medical Director and Consultant Gynaecologist
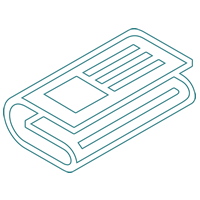
Endometriosis is a condition in which tissue that normally lines the inside of your womb (endometrial cells), grows outside your uterus. The endometrial cells could grow in ovaries, fallopian tubes, bowel, bladder, and lining of your pelvis. On the odd occasion, endometrial tissue may spread beyond pelvic organs to the lungs or skin. Endometriosis can affect any woman of reproductive age, which can be anything between the ages of 15-49 years on average.
The displaced endometrial tissue continues to act as it normally would; it thickens, breaks down, and bleeds with each menstrual cycle. As this displaced tissue cannot exit your body, it becomes trapped. If the endometriosis is in the ovaries it can create a cyst called endometriomas which can irritate the surrounding tissue and eventually develop scar tissue and adhesions. Abnormal bands of fibrous tissue can also cause pelvic tissues and organs to stick to each other, causing tubal blockage or obstruction of the bowels.
A definite cause for endometriosis has not been confirmed. However, several theories have been suggested including:
The main symptom of endometriosis is pelvic pain, often during the menstrual period, typically describe as far worse than usual. Women with endometriosis also tend to report that the pain increases over time.
Other symptoms during your period are fatigue, diarrhea, constipation, bloating, or nausea, especially during menstrual periods.
Endometriosis is sometimes mistaken for other conditions that can cause pelvic pain, such as pelvic inflammatory disease (PID) or ovarian cysts. It may be confused with irritable bowel syndrome (IBS), a condition that causes bouts of diarrhea, constipation, and abdominal cramping. IBS can accompany endometriosis, which can complicate the diagnosis.
Endometriosis usually develops several years after the onset of menstruation (menarche). Signs and symptoms of endometriosis end temporarily with pregnancy and end permanently with menopause, (unless you’re taking estrogen hormone replacement therapy-HRT). It takes on average 7-10 years from the onset of symptoms to diagnosis in many cases. However, with better information, women are getting referred to see specialists earlier. With improving non-invasive ultrasound imaging, early diagnosis is possible, with prompt treatment, resulting in much better outcomes.
There are medical treatments, including painkillers and hormonal tablets or injections which are very effective, especially in pain management. However, they are in some cases contraceptives as well and not suitable for those wishing to conceive.
Surgical removal of endometriosis is mainly performed as a key-hole procedure, laparoscopy. In the vast majority of cases, this is a day surgery procedure. Endometriosis ovarian cysts; blocked and damaged tubes and other pelvic endometriosis lesions can be managed in this way to treat pain and infertility.
The main complication of endometriosis is impaired fertility. Approximately one-third to one-half of women with endometriosis have difficulty getting pregnant.
To conceive, an egg must be released from the ovary, travel through the fallopian tube, become fertilized by a sperm cell within the fallopian tube, start dividing and travel down the fallopian tube over a five-day period before getting into the uterine cavity, and implant into the uterine wall lining to continue its development. Endometriosis may obstruct the tube and keep the egg and sperm from reaching each other and fertilising. The transport of a fertilised egg through the fallopian tubes may also be impeded, with resulting implantation within the fallopian tube, known as an ectopic pregnancy.
Endometriosis also seems to affect fertility in less-direct ways, such as damage to the sperm or egg.
Medication doesn’t always improve fertility. Surgery to remove visible patches of mild to moderate endometriosis tissue can sometimes help. However, in severe cases of endometriosis, the chances of a spontaneous conception are lower. Surgery in severe cases may alleviate the pain symptoms and improve the chances of successful fertility treatment. If you’re having difficulty getting pregnant, infertility treatments, such as in vitro fertilisation (IVF), may be an option.
Even so, many women with mild to moderate endometriosis can still conceive and carry a pregnancy to term. Doctors advise women with endometriosis who wish to have children not to delay having children because the condition may worsen with time.
Ovarian cancer does occur at higher-than-expected rates in women with endometriosis. Thankfully, the overall lifetime risk of ovarian cancer is low, to begin with. Some studies suggest that endometriosis increases that risk, but it’s still relatively low. Although rare, another type of cancer — endometriosis-associated adenocarcinoma — can develop later in life in women who have had endometriosis.
See your GP if you have signs or symptoms of endometriosis, especially if they have a big impact on your quality of life. Your GP will examine you, arrange tests and if endometriosis is suspected, refer you to a specialist.
Our endometriosis and fertility specialists at Herts and Essex Fertility Centre provide advice, investigations, and all forms of endometriosis treatment. You do not require a GP referral to arrange an appointment. Following your appointment, your GP will be kept informed of your investigations and treatment.
Contact our fertility experts on 0199278 50 60 to discuss how we can support you.